Amid the COVID-19 pandemic, extensive research has focused on deep learning methodologies for accurately diagnosing the virus from chest X-ray images. Various models, including Convolutional Neural Networks (CNNs) and pre-trained models, have achieved accuracies ranging from 85.20% to 99.66%. However, the proposed Fine-Tuned ResNet50 model consistently outperforms others with an impressive accuracy of 98.20%. By leveraging on transfer learning and careful architectural design the proposed model demonstrates superior performance compared to previous studies using DarkNet, ResNet50, and pre-trained models. Graphical comparisons highlight its competitive edge, emphasizing its effectiveness in COVID-19 classification tasks. The ResNet50 architecture, known for its deep residual layers and skip connections, facilitates robust feature extraction and classification, especially in medical imaging. Data pre-processing techniques, like noise reduction and contrast enhancement, ensure input data quality and reliability, enhancing the model's predictive abilities. Training results reveal the model's steady accuracy improvement and loss reduction over 20 epochs, aligning closely with validation metrics. Evaluation on a test set of COVID-19 chest X-ray images confirms exceptional accuracy (98.20%), precision (99.00%), recall (98.82%), and F1-score (98.91%), highlighting its proficiency in identifying COVID-19 cases while minimizing false positives and negatives. Comparative analyses against prior studies further validate its superior performance, establishing the Fine-Tuned ResNet50 model as a reliable tool for COVID-19 diagnosis. Future research should focus on exploring ensemble learning techniques, interpretability methods, and stakeholder collaboration to ensure safe AI deployment in clinical settings. Moreover, larger and diverse datasets are crucial for validating model performance and improving generalization, ultimately enhancing patient care and public health outcomes in the mitigating COVID-19 and future pandemics.
| Published in | Machine Learning Research (Volume 9, Issue 1) |
| DOI | 10.11648/j.mlr.20240901.12 |
| Page(s) | 10-25 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Transfer Learning, Deep Learning, COVID-19, Chest X-Ray, ResNet50, Classification
Techniques Used | Year | DL | ML | Hybrid Technique | Dataset | Accuracy |
|---|---|---|---|---|---|---|
Hybrid Deep Transfer Learning [17] | 2023 | √ | X | √ | CXR | Not provided |
CNN [18] | 2020 | √ | X | X | CXR | 98.07% |
Inception V3 [19] | 2020 | √ | X | X | CXR | 97.97% |
ResNet50 [20] | 2021 | √ | X | X | CXR | 98% |
CNN [21] | 2023 | √ | X | X | CXR | 96.66% |
CNN [22] | 2022 | √ | X | X | CXR | 95% |
CNN [23] | 2020 | √ | X | X | CXR | 98.15% |
CNN [24] | 2020 | √ | X | X | CXR | 96.78% |
DarkNet [25] | 2020 | √ | X | X | CXR | 98.08% |
CNN [26] | 2020 | √ | X | X | CXR | 94.70% |
Deep Learning Model [15] | 2022 | √ | X | X | CXR | 97.60% |
ResNet50 [27] | 2020 | √ | X | X | CXR | 98.18% |
ResNet50 [28] | 2021 | √ | X | X | CXR | 84.35% |
EfficientnetB4 [29] | 2022 | √ | X | X | CXR | 97% |
GAN + Deep Transfer Learning [30] | 2020 | √ | X | X | CXR | 85.20% |
Modified DarkCovidNet (CNN) [31] | 2022 | √ | X | X | CXR | 94.18% |
Optimized VGG19 CNN [32] | 2020 | √ | X | X | CXR | 86% |
VGG-CapsNet [33] | 2021 | √ | X | X | CXR | 97% |
Mask R-CNN [11] | 2021 | √ | X | X | CXR | 96.98% |
Improved Deep Learning [35] | 2021 | √ | X | X | CXR | 95.63% |
nCOVnet [34] | 2020 | √ | X | X | CXR | 97.97% |
SVM, DT, RF, ANN [9] | 2022 | X | √ | X | Clinical | 96% |
3.1. Data Collection
3.1.1. Type, Sources and Description of Dataset Utilized
3.1.2. Chest X-Ray Images Dataset
Dataset name | COVID-19 Radiography Database |
Brief description | An open-access dataset with CXR images of COVID-19 positive and negative cases. |
File Size | 816MB |
Source | https://www.kaggle.com/tawsifurrahman/covid19-radiography-database |
Normal images | 10,192 data points |
Positive cases images | 3,616 data points |
Remark | Imbalanced dataset |
3.2. Data Pre-processing
Dataset | CXR |
|---|---|
Total collected | 13,808 |
Blurred Images | 450 |
Balance | 13,358 |
3.3. Data Split Strategy for CXR Dataset
Quality dataset | Training (80%) | Validation (10%) | Testing (10%) |
|---|---|---|---|
13,358 | 10,686 | 1,336 | 1,336 |
3.4. Proposed Model Architectural Design Considerations
3.4.1. ResNet50 Model
3.4.2. Design Consideration for ResNet-50 in Classification of COVID-19 CXR Image Dataset
S/N | Design considerations | Details |
|---|---|---|
1 | Model Architecture | ResNet50 - A deep residual network with 50 layers |
2 | Input Shape | (224, 224, 3) - RGB images resized to 150x150 pixels |
3 | Pre-processing | Data normalization to rescale pixel values to the range [0,1] |
4 | Pre-trained Weights | 'imagenet' - Initialize with weights pre-trained on ImageNet |
5 | Fine-tuning | Fine-tune the pre-trained ResNet50 layers or freeze all layers |
6 | Batch Normalization | Normalize the activations of each layer to speed up training and improve stability |
7 | Dropout | Apply dropout regularization after fully connected layers to prevent overfitting |
8 | Loss Function | Binary Cross-entropy |
9 | Optimizer | Adam optimizer with a learning rate of 0.0001 |
10 | Metrics | Accuracy, Precision, Recall, F1-score |
11 | Batch Size | 64 |
12 | Epochs | 20 |
13 | Early Stopping | Monitor validation loss and stop training if no improvement after a certain number of epochs |
14 | Class Weighting | Adjust class weights to handle class imbalance if necessary |
3.4.3. Training Parameters for ResNet50 on COVID-19 CXR Image Dataset
S/N | Parameter | Values |
|---|---|---|
1 | Batch size | 64 |
2 | Epoch | 20 |
3 | Learning rate | 0.0001 |
4 | Classes | 2 |
5 | Input shape | (150, 150, 3) |
6 | Seed | 42 |
7 | Target size | (150, 150) |
8 | Classes description | ‘Covid’, ‘Normal’ |
9 | Class mode | Binary |
10 | Split percentage for training | 80% |
11 | Split percentage for validation | 10% |
3.4.4. Proposed System Architecture
3.4.5. Mathematical Notation for the Proposed Model
3.4.6. Algorithm Adopted
3.4.7. Experimental Platform Configuration
Configuration | Parameters |
|---|---|
CPU | Intel® Core ™ i7-8700, CPU@3.2 – 4.6GHz |
GPU | NVIDIA GeForce GTX 1080Ti 16GB GDDR5X |
Memory | 64GB DDR4 2133MHz |
Operating System | MS Windows 10 |
Programming Language | Python 3.5 |
Development Platform | Anaconda3 Pycharm Community Edition |
Framework | Tensorflow 10.0 |
3.4.8. Evaluation Metric
4.1. Model Training Results
Epoch | Accuracy | Val_Accuracy | Loss | Val_Loss | Time |
|---|---|---|---|---|---|
1 | 0.74 | 0.80 | 0.56 | 0.39 | 1268s |
2 | 0.77 | 0.75 | 0.45 | 0.44 | 1293s |
3 | 0.79 | 0.86 | 0.43 | 0.36 | 1110s |
4 | 0.81 | 0.87 | 0.40 | 0.33 | 1225s |
5 | 0.81 | 0.81 | 0.39 | 0.37 | 1683s |
6 | 0.83 | 0.87 | 0.37 | 0.31 | 1055s |
7 | 0.84 | 0.88 | 0.35 | 0.30 | 849s |
8 | 0.84 | 0.85 | 0.35 | 0.30 | 846s |
9 | 0.84 | 0.88 | 0.34 | 0.29 | 841s |
10 | 0.84 | 0.87 | 0.35 | 0.33 | 839s |
11 | 0.83 | 0.85 | 0.36 | 0.31 | 836s |
12 | 0.85 | 0.89 | 0.33 | 0.28 | 839s |
13 | 0.86 | 0.85 | 0.32 | 0.32 | 839s |
14 | 0.86 | 0.89 | 0.31 | 0.26 | 835s |
15 | 0.87 | 0.88 | 0.31 | 0.28 | 841s |
16 | 0.86 | 0.88 | 0.31 | 0.29 | 842s |
17 | 0.87 | 0.90 | 0.29 | 0.25 | 834s |
18 | 0.87 | 0.88 | 0.30 | 0.27 | 841s |
19 | 0.86 | 0.86 | 0.30 | 0.30 | 840s |
20 | 0.88 | 0.90 | 0.28 | 0.24 | 834s |
4.2. Model’s Test Results Based on COVID-19 CXR Image Test Sets
4.3. Comparison Evaluation
| [1] | Awwalu J., Umar N. A., Ibrahim M. S., and Ogwueleka F. N. (2020), A Multinomial Naïve Bayes Decision Support System for COVID-19 Detection, FUDMA Journal of Sciences (FJS) 4(2): 704-711. |
| [2] | Sait U, K V GL, Shivakumar S, Kumar T, Bhaumik R, Prajapati S, Bhalla K, and Chakrapani A. (2021). A deep-learning based multimodal system for Covid-19 diagnosis using breathing sounds and chest X-ray images. Appl Soft Comput. 109: 107522. |
| [3] |
World Health Organization. (2020b). COVID-19: The race to find a vaccine. Retrieved from
https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON-24-march-2020 |
| [4] | World Health Organization. (2021). COVID-19 vaccines. Retrieved from |
| [5] | Pola Ö. (2021), Detection of Covid-19 from Chest CT Images Using Xception Architecture: A Deep Transfer Learning Based Approach, Sakarya University Journal of Science, 25(3), 800-810. |
| [6] | Rani G., Oza M. G., Dhaka V. S., Pradhan N., Verma S., and Rodrigues J. P. C. (2022), Applying deep learning based multi modal for detection of coronavirus, Multimedia Systems 28: 1251-1262. |
| [7] | Shikang L., Zhuo L., Ruiqing X., Xiaofeng Y., Jianhua L., Liang L., Yuyan S., Qiangzhong S., Tongxin L., Lanlan Q., and Ying, Z. (2021), Multimodal deep learning for predicting COVID-19 patients at high-risk for serious illness, Electronic Journal of Emerging Infectious Diseases, 6(2): 133-137. |
| [8] | Shahanaz A. G., Niranjana S., Madhushankara M and Swathi K. S. (2022), Deep learning model for detection of COVID-19 utilizing the chest X-ray images, Cogent Engineering, 9(1), 1-18, |
| [9] | Chauha H., and Modi K. (2022), Development of a Multi-modal Severity Prediction System for Covid-19 using Machine Learning Algorithms, International Journal of Intelligent Systems and Applications in Engineering IJISAE, 10(3), 314–321. |
| [10] | Guo H., Zhou Y., Liu X and Tan J. (2020), The impact of the COVID-19 epidemic on the utilization of emergency dental services, Journal of Dental Sciences, 15(4): 564–567. |
| [11] | Soumyajit P, Somnath B., and Arijit R. (2021), An efficient method of detection of COVID-19 using Mask R-CNN on chest X-Ray images, AIMS Biophysics, 8(3): 281–290. |
| [12] | Afreen, Y. N., and Reddy, P. B. (2022). CDLX: An Efficient novel approach for COVİD detection lung xrays throw transfer learning based on State of the art deep learning image classification models. International Journal of Health Sciences, 6(S5): 8439–8463. |
| [13] | Ghomi Z, Mirshahi R, Khameneh B. A, Fattahpour A, Mohammadiun S, Alavi Gharahbagh A, Djavadifar A, Arabalibeik H, Sadiq R, and Hewage K. (2020). Segmentation of COVID-19 pneumonia lesions: A deep learning approach. Medical Journal Islam Republic Iran, 34(174): 1–7, |
| [14] | Subhalakshmi R. T., Balamurugan S A. A., and Sasikala S. (2022), Deep learning based fusion model for COVID-19 diagnosis and classification using computed tomography images, Concurrent Engineering: Research and Applications, 30(1): 116 – 127. |
| [15] | Vedika et al. (2022), Improved COVID-19 detection with chest x-ray images using deep learning, Multimedia Tools and Applications, 2022(81): 37657–37680. |
| [16] | Abbasi-Kesbi, K., Jafari, M. H., & Alizadehsani, R. (2022). A deep neural network model for COVID-19 prediction based on chest CT images. Journal of X-Ray Science and Technology, 30(1), 103-114. |
| [17] | Kaushik, B., Chadha, A. & Sharma, R. (2023), Performance Evaluation of Learning Models for the Prognosis of COVID-19. New Gener. Comput. 41, 533–551. |
| [18] | Purohit, K., Kesarwani, A., Kisku, D. R., & Dalui, M. (2020). COVID-19 Detection on Chest X-Ray and CT Scan Images Using Multi-image Augmented Deep Learning Model. bioRxiv. |
| [19] | Jain, R., Gupta, M., Taneja, S., & Hemanth, D. J. (2020). Deep learning based detection and analysis of COVID-19 on chest X-ray images. Applied Intelligence (Dordrecht, Netherlands), 51, 1690-1700. |
| [20] | Rehman, A., Sadad, T., Saba, T., Hussain, A., & Tariq, U. (2021). Real-Time Diagnosis System of COVID-19 Using X-Ray Images and Deep Learning. IT Professional, 23, 57-62. |
| [21] | Mukri, V. M. (2023), COVID-19 Prediction using Machine Learning, International Research Journal of Modernization in Engineering Technology and Science, 5(3): 1180–1185. |
| [22] | Muhammad et al. (2022), Deep transfer learning CNN based approach for COVID-19 detection, International Journal of Advanced and Applied Sciences, 9(4): 44-52. |
| [23] | Sekeroglu B., and Ozsahin I. (2020), Detection of COVID-19 from Chest X-Ray Images using Convolutional Neural Networks, SLAS Technology, 25(6): 553–565. |
| [24] | Apostolopoulos, I. D., & Mpesiana, T. A. (2020), Covid 19: automatic detection from X ray images utilizing transfer learning with convolutional neural networks, Physical and Engineering Sciences in Medicine, 43, 635-640. |
| [25] | Ozturk, T., Talo, M., Yildirim, E. A., Baloglu, U. B., Yildirim, O., & Acharya, R. U. (2020), Automated detection of COVID-19 cases using deep neural networks with X-ray images, Computers in Biology and Medicine, 121 (103792), 1–11. |
| [26] | Ismael, A. M., & Şengür, A. (2020). Deep learning approaches for COVID-19 detection based on chest X-ray images. Expert Systems with Applications, 164, 114054 - 114054. |
| [27] | Bukhari, S. U., Bukhari, S. U., Syed, A., & Shah, S. S. (2020). The diagnostic evaluation of Convolutional Neural Network (CNN) for the assessment of chest X-ray of patients infected with COVID-19. medRxiv. |
| [28] | Nandi R., and Mulimani M. (2021), Detection of COVID-19 from X-rays using hybrid deep learning models, Research on Biomedical Engineering, 37: 687–695. |
| [29] | Khalil, M. I., Rehman, S. U., Alhajlah, M., Mahmood, A., Karamat, T., Haneef, M., & Alhajlah, A. (2022). Deep-COVID: Detection and Analysis of COVID-19 Outcomes Using Deep Learning. Electronics. |
| [30] | Loey, M., Smarandache, F., & Khalifa, N. E. (2020). Within the Lack of Chest COVID-19 X-ray Dataset: A Novel Detection Model Based on GAN and Deep Transfer Learning. Symmetry, 12, 651. |
| [31] | Redie, D. K., Sirko, A. E., Demissie, T. M., Teferi, S. S., Shrivastava, V. K., Verma, O. P., & Sharma, T. K. (2022). Diagnosis of COVID-19 using chest X-ray images based on modified DarkCovidNet model. Evolutionary Intelligence, 16, 729-738. |
| [32] | Horry, M. J., Chakraborty, S., Paul, M., Ulhaq, A., Pradhan, B., Saha, M., & Shukla, N. (2020). COVID-19 Detection Through Transfer Learning Using Multimodal Imaging Data. Ieee Access, 8, 149808 - 149824. |
| [33] | Shamik T., and Anurag J. (2021), Convolutional capsule network for COVID-19 detection using radiography images, International Journal of Imaging System Technol., 31: 525–539. |
| [34] | Panwar, H., Gupta, P. K., Siddiqui, M. K., Morales-Menendez, R., & Singh, V. (2020), Application of deep learning for fast detection of COVID-19 in X-Rays using nCOVnet, Chaos, Solitons and Fractals, 138 (109944), 1–8. |
| [35] | Bashar, A., Latif, G., Ben-Brahim, G., Mohammad, N., and Alghazo, J. (2021), COVID-19 Pneumonia Detection Using Optimized Deep Learning Techniques. Diagnostics, 11, 1 - 18. |
APA Style
Dokun, O., John-Otumu, A. M., Eze, U. F., Ikerionwu, C., Etus, C., et al. (2024). Deep Learning Model for COVID-19 Classification Using Fine Tuned ResNet50 on Chest X-Ray Images. Machine Learning Research, 9(1), 10-25. https://doi.org/10.11648/j.mlr.20240901.12
ACS Style
Dokun, O.; John-Otumu, A. M.; Eze, U. F.; Ikerionwu, C.; Etus, C., et al. Deep Learning Model for COVID-19 Classification Using Fine Tuned ResNet50 on Chest X-Ray Images. Mach. Learn. Res. 2024, 9(1), 10-25. doi: 10.11648/j.mlr.20240901.12
AMA Style
Dokun O, John-Otumu AM, Eze UF, Ikerionwu C, Etus C, et al. Deep Learning Model for COVID-19 Classification Using Fine Tuned ResNet50 on Chest X-Ray Images. Mach Learn Res. 2024;9(1):10-25. doi: 10.11648/j.mlr.20240901.12
@article{10.11648/j.mlr.20240901.12,
author = {Oyewole Dokun and Adetokunbo Macgregor John-Otumu and Udoka Felista Eze and Charles Ikerionwu and Chukwuemeka Etus and Emeka Matthew Nwanga and Ogadimma Thaddeus Okonkwo},
title = {Deep Learning Model for COVID-19 Classification Using Fine Tuned ResNet50 on Chest X-Ray Images
},
journal = {Machine Learning Research},
volume = {9},
number = {1},
pages = {10-25},
doi = {10.11648/j.mlr.20240901.12},
url = {https://doi.org/10.11648/j.mlr.20240901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.mlr.20240901.12},
abstract = {Amid the COVID-19 pandemic, extensive research has focused on deep learning methodologies for accurately diagnosing the virus from chest X-ray images. Various models, including Convolutional Neural Networks (CNNs) and pre-trained models, have achieved accuracies ranging from 85.20% to 99.66%. However, the proposed Fine-Tuned ResNet50 model consistently outperforms others with an impressive accuracy of 98.20%. By leveraging on transfer learning and careful architectural design the proposed model demonstrates superior performance compared to previous studies using DarkNet, ResNet50, and pre-trained models. Graphical comparisons highlight its competitive edge, emphasizing its effectiveness in COVID-19 classification tasks. The ResNet50 architecture, known for its deep residual layers and skip connections, facilitates robust feature extraction and classification, especially in medical imaging. Data pre-processing techniques, like noise reduction and contrast enhancement, ensure input data quality and reliability, enhancing the model's predictive abilities. Training results reveal the model's steady accuracy improvement and loss reduction over 20 epochs, aligning closely with validation metrics. Evaluation on a test set of COVID-19 chest X-ray images confirms exceptional accuracy (98.20%), precision (99.00%), recall (98.82%), and F1-score (98.91%), highlighting its proficiency in identifying COVID-19 cases while minimizing false positives and negatives. Comparative analyses against prior studies further validate its superior performance, establishing the Fine-Tuned ResNet50 model as a reliable tool for COVID-19 diagnosis. Future research should focus on exploring ensemble learning techniques, interpretability methods, and stakeholder collaboration to ensure safe AI deployment in clinical settings. Moreover, larger and diverse datasets are crucial for validating model performance and improving generalization, ultimately enhancing patient care and public health outcomes in the mitigating COVID-19 and future pandemics.
},
year = {2024}
}
TY - JOUR T1 - Deep Learning Model for COVID-19 Classification Using Fine Tuned ResNet50 on Chest X-Ray Images AU - Oyewole Dokun AU - Adetokunbo Macgregor John-Otumu AU - Udoka Felista Eze AU - Charles Ikerionwu AU - Chukwuemeka Etus AU - Emeka Matthew Nwanga AU - Ogadimma Thaddeus Okonkwo Y1 - 2024/05/10 PY - 2024 N1 - https://doi.org/10.11648/j.mlr.20240901.12 DO - 10.11648/j.mlr.20240901.12 T2 - Machine Learning Research JF - Machine Learning Research JO - Machine Learning Research SP - 10 EP - 25 PB - Science Publishing Group SN - 2637-5680 UR - https://doi.org/10.11648/j.mlr.20240901.12 AB - Amid the COVID-19 pandemic, extensive research has focused on deep learning methodologies for accurately diagnosing the virus from chest X-ray images. Various models, including Convolutional Neural Networks (CNNs) and pre-trained models, have achieved accuracies ranging from 85.20% to 99.66%. However, the proposed Fine-Tuned ResNet50 model consistently outperforms others with an impressive accuracy of 98.20%. By leveraging on transfer learning and careful architectural design the proposed model demonstrates superior performance compared to previous studies using DarkNet, ResNet50, and pre-trained models. Graphical comparisons highlight its competitive edge, emphasizing its effectiveness in COVID-19 classification tasks. The ResNet50 architecture, known for its deep residual layers and skip connections, facilitates robust feature extraction and classification, especially in medical imaging. Data pre-processing techniques, like noise reduction and contrast enhancement, ensure input data quality and reliability, enhancing the model's predictive abilities. Training results reveal the model's steady accuracy improvement and loss reduction over 20 epochs, aligning closely with validation metrics. Evaluation on a test set of COVID-19 chest X-ray images confirms exceptional accuracy (98.20%), precision (99.00%), recall (98.82%), and F1-score (98.91%), highlighting its proficiency in identifying COVID-19 cases while minimizing false positives and negatives. Comparative analyses against prior studies further validate its superior performance, establishing the Fine-Tuned ResNet50 model as a reliable tool for COVID-19 diagnosis. Future research should focus on exploring ensemble learning techniques, interpretability methods, and stakeholder collaboration to ensure safe AI deployment in clinical settings. Moreover, larger and diverse datasets are crucial for validating model performance and improving generalization, ultimately enhancing patient care and public health outcomes in the mitigating COVID-19 and future pandemics. VL - 9 IS - 1 ER -
Department of Information Technology, Federal University of Technology, Owerri, Nigeria
Department of Information Technology, Federal University of Technology, Owerri, Nigeria
Department of Information Technology, Federal University of Technology, Owerri, Nigeria
Department of Software Engineering, Federal University of Technology, Owerri, Nigeria
Department of Information Technology, Federal University of Technology, Owerri, Nigeria
Department of Information Technology, Federal University of Technology, Owerri, Nigeria
Department of Information Technology, Federal University of Technology, Owerri, Nigeria
Figure 1. Picture of B.1.351 (South African Variant) [3].
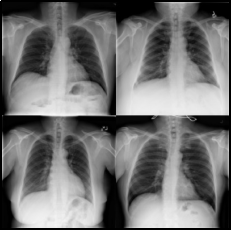
Figure 3. Sample Normal CXR images (Kaggle.com).
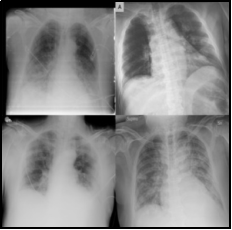
Figure 4. Sample Positive COVID-19 Chest X-ray images (Kaggle.com).
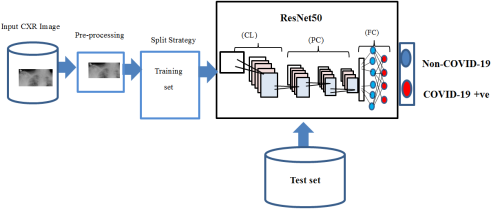
Figure 5. Proposed system architecture for COVID-19 Classification.
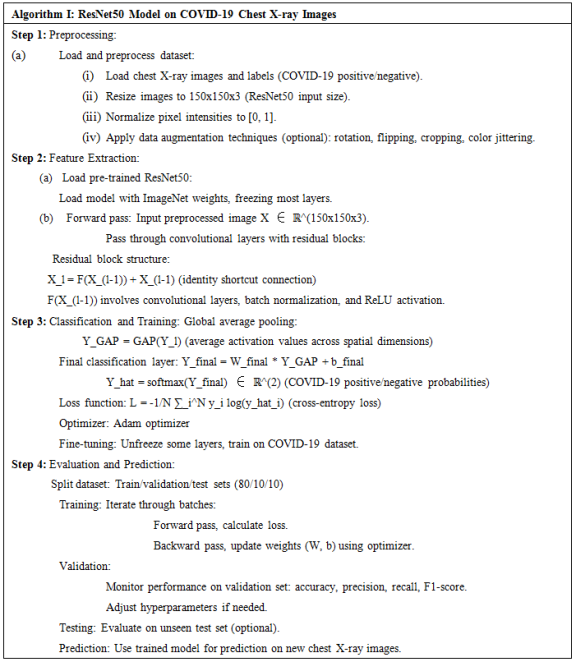
Figure 6. ResNet50 Algorithm on COVID-19 CXR image.
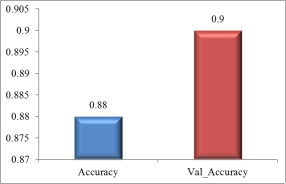
Figure 7. Tradeoff between accuracy and validation accuracy on training set.
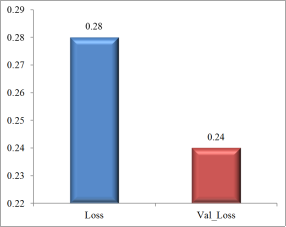
Figure 8. Tradeoff between loss and validation loss on training set.
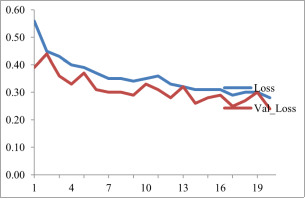
Figure 9. Visualization of training loss based on ResNet50 on COVID-19 CXR training set.
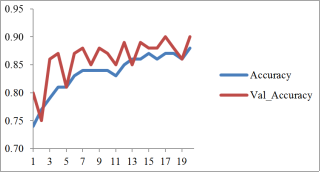
Figure 10. Visualization of training accuracy based on ResNet50 using COVID-19 CXR training set.
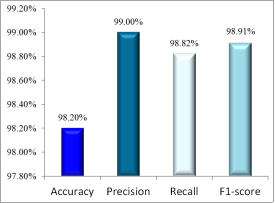
Figure 11. Graphical representation of the test set results.
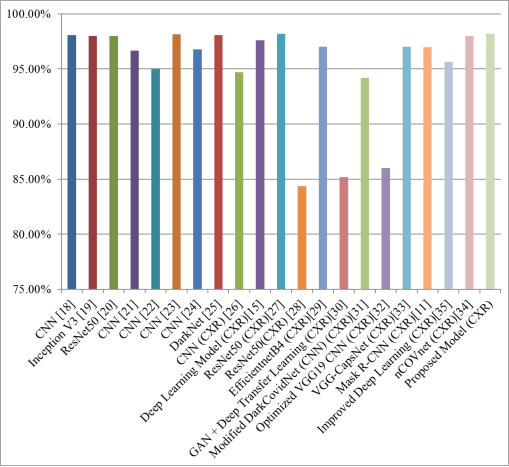
Figure 12. Comparison between selected previous studies and the proposed model.

